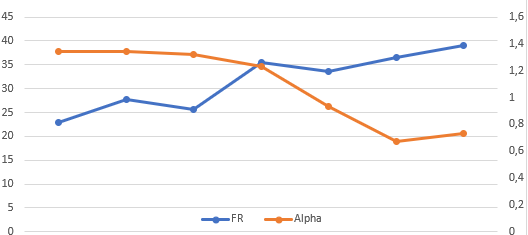
When alpha drops so fast it can mean, if there are no intensities to justify it, a fatigue in the autonomic nervous system (ANS).
1 Like
Very tough intervals  100% Vo2Max to reach 95% HRMAX which is about 2 minutes.
100% Vo2Max to reach 95% HRMAX which is about 2 minutes.
@MedTechCD Just wanted to share w/ you something I was playing with since I got my H10.
Took me a couple of days to figure out how to get the ECG data from the Polar. It wasn’t easy esp since I didn’t want to utilise Polar’s SDK (They’re using a library; RxSwift which I am totally not versed on). Then I had to muddle thru their SDK documentation (somehow Bluetooth’s spec documentation is bad compare to ANT+) and code and do a series of trial and error.(Many many head banging  )
)
So, finally I have something to show for it.

The 2nd Plot truncates the initial ~500 points. Initial goal is just to get the Peak to Valley range so I get good HRV data.
5 Likes
Nice and clean ECG!
Thanks to this thread and my colleague @MedTechCD I learned that “Fatmaxxer” creates ECG records but only for fragments where errors occurred.
Because for several weeks I have been observing my heart’s suspicious behavior (I feel like choking and “stuffing” with pressure under the lattice at the same time).
“Fatmaxxer” signaled each such episode as “three artifacts” or “two artifacts”. I was able to find out the differences between them when I created a graph in Excel based on the ECG records.
For me, “triple artifact” means shortening one heartbeat and lengthening the next (as if in a pattern instead of the normal 2 - 2, there was a stroke in the 1 - 3 pattern). “Fatmaxxer” is represented in a pink graph as a downward tilt followed by an upward bounce crossing the midline and back to the middle position from the maximum excursion.
On the other hand, “double artifact” is just the “top half of the graph” shoots up sharply and drops to its level (does not go down).
On the EKG, this second episode looks … dramatic: /
From a conversation with a friend it appears that this is … an arrhythmia.
Tomorrow I have an appointment with a cardiologist and, just in case, I also arranged an exercise test (if the cardiologist recommends it).
These are my errors:
 - trening")
(there is a window from “Fatmaxxer”)
BTW - if it weren’t for the Polar H10, “Fatmaxxer”, this thread and my inquisitiveness, I would have no idea that something is wrong with my heart.
regards
Artur
Which file is this in when you download them from Fatmaxxer?
@Cary_Blackburn - the question you put to me?
If so, “Fatmaxxer” saves 3 or 4 files.
The first basic one is a file with the annotation “features” - it includes parameters such as date / time, HR, rmSSD, SDNN, alphav1, alphav2, artifacts, samples, threshold. It’s a csv file - so easy to manipulate.
The second basic file is a file with the annotation “RR” - in addition to the date / time, the “R-R” parameters are saved.
The third file is with the note “DEBUG” and the log extension. I do not know what its use is, but I suspect that it is useful for the developer for possible error analysis with the application.
Natoamist, the fourth file is created when there is a so-called “artifact”, i.e. an irregularity, or with an extension of, for example, a signal drop, loss of communication or medical reasons (heart defect?).
This file has an annotation “ECG” and a csv spread - so easy to process.
It contains the ECG record for ~ 10-13 seconds in the vicinity of the “artifact”, which allows to assess whether the artifact has a purely technical, communication or medical basis (arrhythmia, excess shocks, etc.).
greetings
Artur
1 Like
I am using H10 + Edge 530 + AlphaHRV over ANT+
Not many artefacts. Still testing if the value is reasonable.
Many thanks for your excellent and complete reply. Much appreciated.
The ecg file is only recorded when the option is activated in Fatmaxxer. There is one csv file with multiple sections. First section is a 10 sec baseline ecg at start, the following sections are about 10 sec around every detected artifact. You can find a guide to plot them here:
1 Like
I added “Avg EPOC” as an interval field. You need to do Action → Reanalyse to see it.
2 Likes
Marco is giving a hard time to HRV while on activities in special on DFA a1
2 Likes
3 Likes
Strong words about DFA
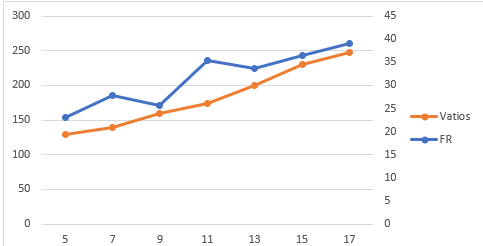
We have been working for some time on personal thresholds, lactate has the same problem, not everyone is 2 mmol or 4mmol, everyone has their personal thresholds, with DFA the same thing happens, another thing is the conflicts of interest that some have, Seiler defends his polarised model that does not work well for everyone, no model is perfect, but we must contribute instead of destroying. DFA has a great future and the research groups will end up bringing it out. I personally am collaborating. Here is an image where you can clearly see the entrance of the first threshold (verified with laboratory test).
3 Likes
@Luisma_Gallego_Soy_P I saw there is a podcast on your work with dfa but it is in Spanish. Is there someplace a summary in English?
I would like to follow-up on what you’re doing because I also believe that there is a future for dfa. It is quite obvious that dfa can be an intensity metric and in a better way then HR alone.
I do however not believe in the fact that Seiler would be driven by a conflict of interest. That doesn’t sound like him at all… Neither from Marco. I think they just want to warn people that it is not yet the moment to blindly follow the conclusions drawn by very limited research untill now.
2 Likes
I am one of those who think that DFA must be careful and know how it works and how it behaves, the thresholds still need a lot of research, but it is true that there is a change when we are at the first threshold (does not have to be 0.75), I for example after covid my threshold with DFA has moved to 1.19, we are creating a python script to detect these jumps of DFA, like a lactate test to set custom thresholds for each one. Currently working on the basis of alpha values is a very big mistake and if someone is doing it I think they are doing it wrong. DFA can be a great metric to check internal load as well. I don’t know if you can add subtitles to the podcast, I’ll check it out.
1 Like
Pardon my ignorance, but what are Vatios & FR?
Vatios=power and FR=Respiratoria rate
2 Likes
Hi guys I’m new here,and have been running for 40 odd yrs .The last 10 yrs using Maffetones 180-age and now using fatmaxxer since launch
.
If accurate Fatmaxxer is saying I’ve been running the start of my long runs too fast(even though low heart rate)and the end of long runs too slow .So if fresh my long runs are now acceleration runs.
One question I would like to know can you just use fatmaxxer to guide you in real time or must you do a ramp test,and if our systems are different depending on fatigue levels etc what is the purpose of the ramp test as on each occasion?